Hospital Air Duct Cleaning and HAI Prevention: What Every Infection Control Professional Should Know
Contaminated HVAC ductwork is a documented reservoir for nosocomial pathogens, yet ventilation hygiene remains one of the most consistently deferred components of hospital infection control programs. Hospital air duct cleaning is not a standalone infection-control measure, but it is a necessary component of the layered engineering controls that keep immunocompromised patients, post-surgical patients, and staff in defensible risk environments.
This guide is written for infection control officers, facility directors, and clinical administrators who need a clear framework for where duct hygiene fits within their broader HAI prevention strategy, what the regulatory standards actually require, and what a compliant cleaning protocol looks like in practice.
CDC data from 2022 estimates 687,000 HAIs occur in U.S. acute care hospitals annually, underscoring the scale of the nosocomial infection burden.
HVAC Systems Are a Documented Nosocomial Pathogen Vector
A hospital's air conveyance system moves up to 30 cubic feet of air per minute through its duct network. That volume is necessary for maintaining the pressure relationships, air change rates, and temperature control that clinical environments require. It also means that any contaminants present in the ductwork circulate continuously through patient rooms, procedure spaces, and critical care units.
The CDC's 2022 National Healthcare-Associated Infections Prevalence Survey estimated 687,000 HAIs in U.S. acute care hospitals in a single year, with approximately 72,000 patient deaths attributed to those infections during hospitalization. While HAIs arise from multiple vectors, ventilation system hygiene is an established environmental risk factor, particularly for fungal and airborne bacterial pathogens. (Source: CDC National and State Healthcare-Associated Infections Progress Report)
Dust accumulation inside ducts creates a substrate for microbial proliferation. Human skin cells, linen fibers, hair, and aerosolized particulate matter deposit on duct surfaces and provide nutrients for bacterial and fungal growth. Moisture in drain pans, coil sections, and humidification components supports biofilm development. Once established, biofilms are significantly harder to remediate than surface-level contamination and can release viable organisms into the airstream during routine system operation.
"Unclean HVAC interiors can trap dust and retain moisture, allowing biofilms or mold to develop. If dislodged, particles can move downstream." — IAQ Restoration USA, Healthcare Facility Duct Cleaning Guidelines
The pathogens of greatest clinical concern in this context include Aspergillus fumigatus and related species in units serving immunocompromised patients, Legionella pneumophila in water-adjacent cooling and humidification components, and airborne dispersal of MRSA and Clostridioides difficile spores through contaminated return air systems. Each of these organisms has been associated with healthcare-acquired disease outbreaks linked to ventilation system deficiencies.
Zone-Specific Risk Stratification: Not All Clinical Areas Carry Equal Ventilation Risk
Effective hospital air duct cleaning programs are not calendar-driven. They are risk-stratified by clinical zone, patient acuity, and air system configuration. ASHRAE Standard 170 establishes the minimum ventilation parameters for each zone type, and those parameters define the performance envelope within which a clean duct system must operate.
Operating Rooms require a minimum of 20 total air changes per hour, positive pressure relative to adjacent corridors, and HEPA filtration. Any duct system serving an OR that fails to maintain laminar or unidirectional airflow due to debris accumulation creates direct perioperative infection risk. Post-construction and post-renovation duct cleaning before OR re-occupancy is a standard precaution precisely because particulate contamination from building work is incompatible with the sterile field.
Airborne Infection Isolation (AII) Rooms operate under negative pressure with a minimum of 12 ACH and require exhaust directed to the exterior or through HEPA filtration before recirculation. Contaminated ductwork in AII systems can compromise directional airflow integrity, which is the primary engineering control for preventing cross-contamination to adjacent spaces.
HSCT and Oncology Units represent the highest-acuity ventilation environment in most facilities. Patients in these units have severely compromised immune function, and even low-level Aspergillus spore exposure can precipitate invasive aspergillosis, a condition carrying mortality rates of 30 to 90 percent in this population. These units require a minimum of 12 ACH, sustained positive pressure, and HEPA filtration. The clinical margin for ventilation failure here is effectively zero.
ICUs require a minimum of 6 ACH of outside air and benefit from positive pressure, though pressure relationships vary by unit design and patient population. Post-surgical and trauma patients in the ICU represent a high-risk population for opportunistic infection, and duct hygiene in these areas warrants more frequent assessment than general ward spaces.
General Patient Rooms carry the lowest minimum ventilation threshold under ASHRAE 170, with 2 ACH of outside air required. Risk stratification still applies: rooms serving patients with respiratory conditions, extended stays, or post-procedural status warrant higher maintenance priority than short-stay or ambulatory care spaces.
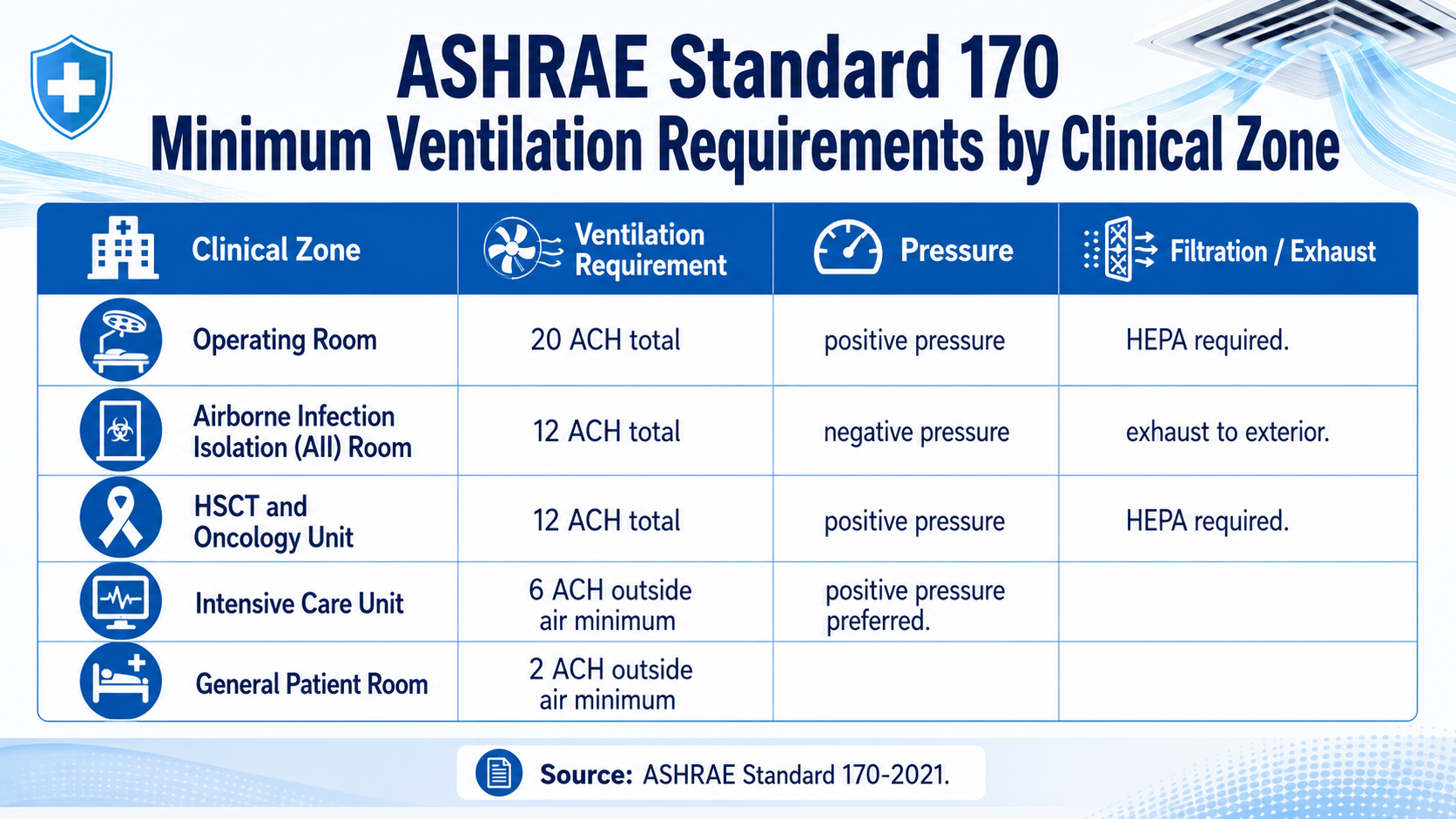
ASHRAE Standard 170 establishes minimum ventilation rates and pressure relationships by clinical zone, forming the baseline against which HVAC system performance is measured.
What Accumulates in Hospital Ductwork and Why It Matters Clinically
Hospital environments generate a specific and clinically relevant contamination profile inside duct systems. Understanding what accumulates and under what conditions informs both cleaning frequency decisions and the urgency of post-incident remediation.
Flexible return duct sections accumulate lint, linen fibers, and fine particulate at a significantly higher rate than rigid ductwork due to their corrugated interior surface. These sections are disproportionately represented in HAI-associated ventilation failures and should receive priority assessment during any inspection.
Drain pans beneath cooling coils are the most common site of Legionella colonization within an HVAC system. Standing water or inadequate drainage creates conditions for biofilm formation within days of a maintenance lapse. Coil surfaces themselves develop fouling layers that reduce thermal transfer efficiency and provide a colonization substrate for fungal organisms.
"Duct accumulation in hospital HVAC systems provides an available food source for bacteria to proliferate. Extra care is required to ensure contaminants are not spread throughout the building envelope during the cleaning process." — Pure Air Control Services, Hospital Duct Cleaning Guidance
In the context of renovation and construction, a 2024 PMC-published study from Ghent University Hospital found that standard in-room duct cleaning using internal brushing methods significantly increased airborne concentrations of Aspergillus fumigatus and A. nidulans during the procedure itself. Particle counts in affected rooms peaked during cleaning and required approximately one hour to return to baseline. (Source: PMC — Improving Ventilation Hygiene in Wards for Immunocompromised Patients, 2025) External duct access methodology, by contrast, produced no significant increase in airborne particle levels. This finding has direct implications for how cleaning is scheduled and performed in occupied wards housing vulnerable patients.
How Hospital Air Duct Cleaning Differs from Commercial Cleaning
Hospital air duct cleaning follows a fundamentally different protocol than standard commercial HVAC maintenance. The distinction is not primarily technical. It is procedural and risk-managed in ways that general commercial contractors are not equipped to execute in clinical environments.
Containment and negative pressurization are non-negotiable during any access to a clinical duct system. Physical barriers isolate the work area from occupied patient spaces, and negative air pressure within the containment zone captures dislodged particulate before it can migrate downstream. HEPA-filtered collection equipment removes captured material at the point of extraction.
Access methodology in occupied wards should follow external-access protocols wherever possible, as supported by the Ghent University Hospital data. Where in-room access is required, the procedure should be coordinated with the infection control officer and scheduled during periods of lowest patient acuity in the affected zone.
Phased, sectional execution maintains ventilation continuity throughout the cleaning program. Hospital air duct cleaning in active clinical facilities must proceed in sections, with each section returned to full function before the next is isolated. This requires pre-planning in coordination with facilities engineering and nursing leadership.
Post-cleaning verification distinguishes compliant hospital-grade service from general commercial work. Verification protocols include visual inspection with photographic or video documentation, particle count measurement before and after cleaning in critical zones, and microbial air sampling where indicated by facility policy or post-incident protocol. Results are documented and retained for Joint Commission Environment of Care compliance records.
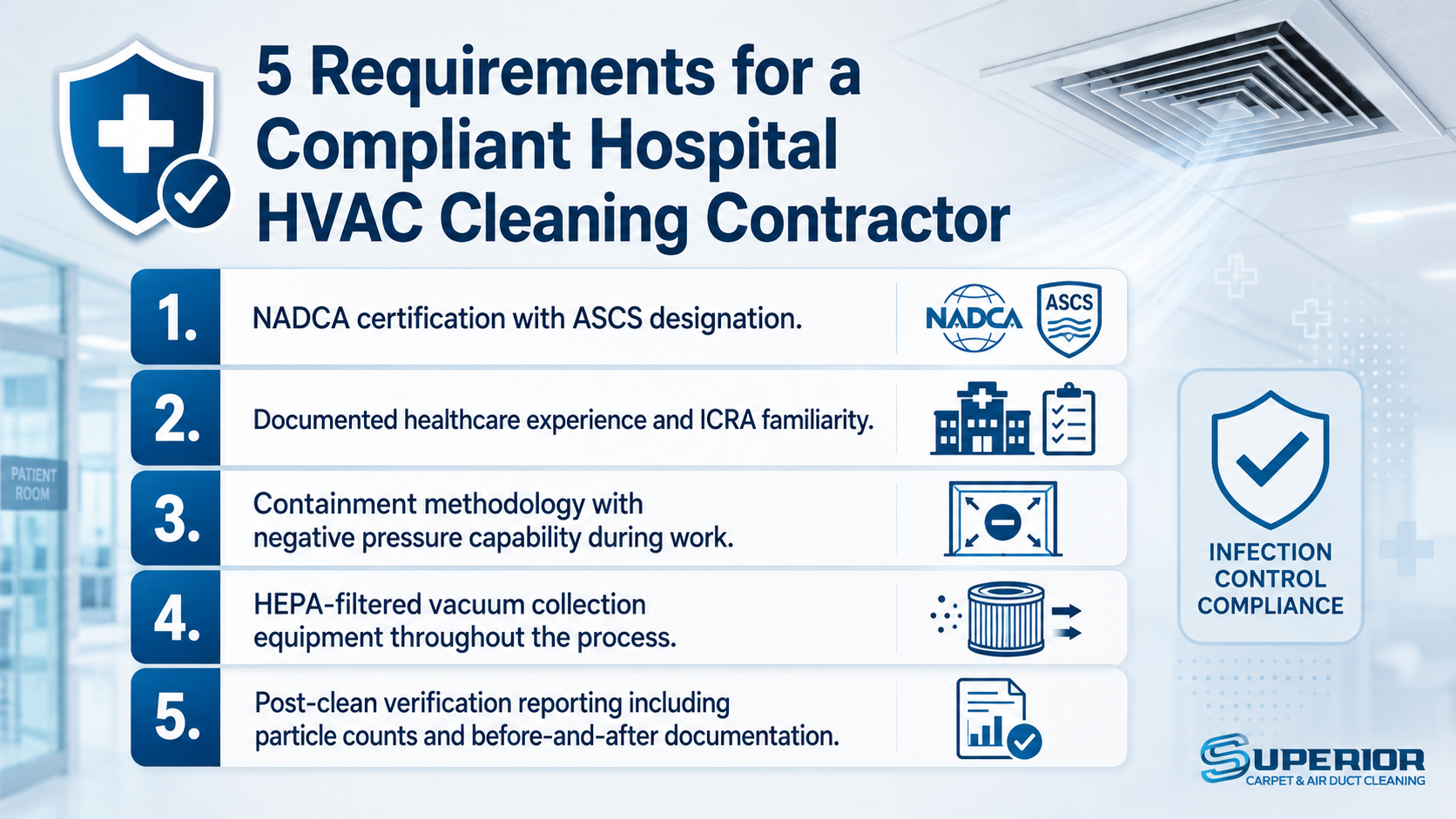
These five criteria help infection control officers and facility directors evaluate HVAC cleaning contractors for clinical environment compliance.
The ICRA Connection: Integrating Duct Hygiene with Your Infection Control Framework
The Infection Control Risk Assessment (ICRA) is the standard pre-construction and pre-renovation tool used to classify activity risk and establish the engineering controls required to protect patients during building work. Most facilities apply ICRA rigorously to construction projects but apply it inconsistently to routine HVAC maintenance.
The Joint Commission's Environment of Care standard EC.02.06.05 addresses infection control during maintenance activities, and its application to duct cleaning is well within scope. Facilities that document ICRA review as part of their hospital air duct cleaning scheduling demonstrate a proactive compliance posture that withstands accreditation scrutiny.
The updated NADCA Assessment, Cleaning and Restoration of HVAC Systems standard (ACR 2025) formalizes an assessment-first methodology: inspect, characterize contamination levels, then clean based on documented findings rather than fixed calendar intervals. For healthcare facilities, this means that annual inspection of air-handling units and critical area supply and return ductwork should drive the cleaning schedule, with high-risk zones assessed more frequently and cleaned whenever contamination levels exceed the facility's established threshold.
Post-incident cleaning, triggered by disease outbreak, water intrusion, or significant construction dust event, should be treated as a separate protocol from routine maintenance and executed under emergency ICRA classification with full containment and verification requirements.
What to Require from Your HVAC Cleaning Contractor
Not all HVAC cleaning contractors have the training, equipment, or protocol familiarity to work safely in clinical environments. Engaging an underqualified vendor in a healthcare setting introduces contamination risk during the cleaning process itself, as the Ghent University data makes clear.
The minimum qualifications for a hospital HVAC cleaning contractor are NADCA certification with at least one Air System Cleaning Specialist (ASCS) credential on the project team, documented experience in healthcare facility environments, demonstrated familiarity with ICRA and Joint Commission Environment of Care standards, containment methodology with verified negative pressure capability, HEPA-filtered vacuum collection equipment throughout all phases of work, and a post-clean verification reporting package that includes particle counts and before-and-after documentation suitable for compliance recordkeeping.
Superior Carpet and Air serves commercial and healthcare facilities across Boise, Meridian, Nampa, Eagle, and the wider Treasure Valley. Our air duct cleaning service uses modern negative-pressure equipment and HEPA-filtered collection systems. We coordinate directly with facility engineering teams to plan phased access, schedule around operational requirements, and deliver documentation that supports your compliance records. See our commercial air duct cleaning services.
Ventilation Hygiene Belongs in Your Infection Control Program
HAI prevention requires layered engineering controls. Surface disinfection, hand hygiene protocols, and instrument sterilization address the pathogen vectors that are visible and immediately accessible. Hospital air duct cleaning addresses the one that moves through the ceiling and into every occupied space in the facility, continuously, 24 hours a day.
The evidence base supports including HVAC hygiene as a documented component of your infection control program, aligned with ICRA protocols, ASHRAE 170 ventilation requirements, and the NADCA ACR 2025 assessment standard. The clinical risk of deferring it is not theoretical.
Schedule a facility assessment with Superior Carpet and Air. We serve healthcare and commercial facilities throughout the Treasure Valley and bring the equipment, documentation, and coordination experience that clinical environments require.
Frequently Asked Questions About Hospital Air Duct Cleaning
How often should hospital air ducts be cleaned?
Cleaning frequency should be driven by inspection findings and zone risk classification, not fixed calendar intervals. NADCA's ACR 2025 standard recommends annual inspection of air-handling units and critical-area supply and return ductwork, with cleaning triggered when contamination exceeds established thresholds. High-acuity zones including ORs, HSCT units, and AII rooms warrant more frequent assessment. Emergency cleaning should follow any outbreak event, water intrusion, or significant construction dust incident regardless of the scheduled maintenance cycle.
What pathogens are most commonly associated with hospital HVAC systems?
Aspergillus fumigatus and related species are the primary fungal concern, particularly in units serving immunocompromised patients. Legionella pneumophila colonizes standing water in drain pans and humidification components. Bacterial organisms including MRSA and Clostridioides difficile can disperse through contaminated return air systems. Each of these organisms has been linked to healthcare-acquired infection outbreaks in facilities with documented ventilation system deficiencies.
Does hospital air duct cleaning reduce HAIs?
Duct cleaning supports HAI prevention as a component of a layered infection control strategy, but it is not a standalone intervention. Contaminated ductwork creates conditions that undermine the performance of filtration, pressure relationships, and air change rates that clinical environments depend on. Maintaining clean duct systems ensures those engineering controls perform as designed. Facilities should document duct hygiene as part of the broader infection control program rather than treating it as an independent clinical intervention.
What standards govern hospital HVAC cleaning?
The primary standards are ASHRAE Standard 170 (ventilation requirements by clinical zone), NADCA's Assessment, Cleaning and Restoration of HVAC Systems standard (ACR 2025), and the Joint Commission's Environment of Care standards EC.02.05.01 and EC.02.06.05. CDC Guidelines for Environmental Infection Control in Health-Care Facilities provide additional evidence-based guidance. Facilities should verify that their cleaning protocols align with the most current versions of each standard, as NADCA released an updated ACR edition in 2025.
How is hospital air duct cleaning different from standard commercial duct cleaning?
Healthcare-grade duct cleaning requires physical containment barriers, negative pressurization of the work zone, HEPA-filtered vacuum collection throughout all phases, phased and sectional execution to maintain ventilation continuity, coordination with infection control and facilities engineering, and post-clean verification with particle counts and documentation suitable for accreditation records. Standard commercial methods do not meet these requirements and introduce contamination risk if applied in occupied clinical spaces.
What is an ICRA and how does it apply to duct maintenance?
An Infection Control Risk Assessment (ICRA) classifies the infection risk associated with maintenance or construction activity and defines the engineering controls required to protect patients during that work. ICRA is standard for construction and renovation projects and is directly applicable to routine HVAC maintenance under Joint Commission EC.02.06.05. Facilities that conduct an ICRA review as part of hospital air duct cleaning scheduling establish a defensible compliance record and reduce the risk of inadvertent patient exposure during the cleaning process.
Can HVAC systems spread airborne pathogens between patient rooms?
Yes, under specific failure conditions. Compromised pressure relationships, blocked or contaminated dampers, and inadequate air change rates can allow airborne pathogens to migrate between zones. AII rooms depend on negative pressure differentials to contain airborne infectious agents, and any duct deficiency that disrupts that differential degrades the primary engineering control for preventing cross-transmission. Regular inspection and hospital air duct cleaning help ensure that the system maintains the pressure relationships and airflow performance that infection control protocols rely on.
What should facilities look for in a hospital HVAC cleaning contractor?
Minimum qualifications include NADCA certification with an ASCS-credentialed technician on the project team, documented healthcare facility experience, ICRA familiarity, containment methodology with negative pressure capability, HEPA-filtered collection equipment, and a post-clean verification package that includes particle counts and before-and-after documentation for compliance recordkeeping. Contractors should also be prepared to coordinate directly with the facility's infection control officer and engineering department throughout the project.
Want to Learn More About Hospital Air Duct Cleaning?
What Is the NADCA ACR Standard?
The NADCA Assessment, Cleaning and Restoration of HVAC Systems standard, updated in 2025, establishes the methodology for inspecting and cleaning air conveyance systems in commercial and institutional settings. The ACR standard requires an assessment-first approach: technicians inspect and document contamination levels before cleaning begins, then execute source removal under conditions that prevent dispersal. For healthcare facilities, ACR compliance is the baseline expectation for any contracted HVAC cleaning work.
How Does ASHRAE Standard 170 Apply to Infection Control?
ASHRAE Standard 170 specifies minimum ventilation rates, pressure relationships, filtration requirements, and air change rates for each clinical zone type in a healthcare facility. These parameters define the performance envelope within which a clean and properly maintained HVAC system must operate. When duct accumulation degrades airflow or compromises filtration effectiveness, the system can no longer meet Standard 170 requirements, and the infection control engineering controls that depend on those parameters are correspondingly compromised.
What Is Biofilm and Why Does It Matter in HVAC Systems?
Biofilm is a structured community of microorganisms that adheres to surfaces and is encased in a self-produced protective matrix. In HVAC drain pans, coil surfaces, and humidification components, biofilm provides a stable reservoir for pathogens that is significantly more resistant to disinfection than planktonic organisms. Legionella pneumophila, in particular, is known to colonize and persist in HVAC biofilms. Source removal during hospital air duct cleaning disrupts biofilm reservoirs at points of formation rather than allowing them to persist between filter change cycles.
How Does Construction Activity Affect Hospital Duct Contamination?
Renovation and construction generate substantial volumes of fine particulate matter, including fungal spores from disturbed materials, that can infiltrate a hospital's air conveyance system if containment controls are inadequate. Post-construction duct cleaning before re-occupancy of affected zones is a standard infection control precaution, particularly in areas adjacent to or served by the same air-handling units as high-acuity clinical spaces. ICRA classification of construction activity directly informs the scope of post-construction duct cleaning required. Learn more about Superior's commercial air duct cleaning services.